A new contribution to the knowledge of Adolescent Idiopathic Scoliosis (AIS)
Antonio Ferrante1, Alberto Ferrante2, Claudia Ferrante3
1 Medico Chirurgo, Spec. in Odontostomatologia, prof. Master in Posturologia clinica Univ. Pisa, Federico II Napoli 2 Medico Chirurgo, spec. in Medicina fisica e riabilitativa , 3 Fisioterapista
Keywords:
Scoliosis, Melatonin, Serotonin, Pineal gland, Trigeminus nerve, Incorrect swallow.
Abstract
Introduction. The problem of idiopathic scoliosis is extremely complex and evaluated in different and discordant ways by the various specialists. All authors agree on one thing: the aethiology of adolescent idiopathic scoliosis still now, after many years of research and studies, is unknown! [1] Theories on AIS’s aethiology have included mechanical, metabolic, hormonal, neuromuscular, growth, and genetic abnormalities. Amongst these, some factors may be epiphenomena rather than the cause itself. [1] Objective. Our research started from completely different bases, compared to specialized orthopedic studies, but perhaps, the possibility of looking for an explanation starting from a “clean slate”, without any preconception, it allowed us to bring a partly new vision, based on our knowledge and skills, different from orthopedic ones. we wanted to show that many scoliosis find their origin in swallowing dysfunction. Methods. Our work was based on the use of devices suitable for measuring orofacial muscles (Myometer), muscle tone (surface electromyography), urinalysis to evaluate the catabolites of neuromediators and hormones produced. The results help to understand the mechanisms through which Scoliosis is created and worsened and indicate a way for its control and often its improvement. WORKING GROUP: N = 40 subjects aged 18-25 years not suffering from diseases of the spine, submitted to postural basic examination and electromyography at rest.
Rescreened with the same parameters after placement of the tongue at the level of the spot Palatine (emergence of the nasal-palatine nerve)
CONTROL GROUP: The same 40 patients constituted the control group, examined after the underlying condition, with different positioning of the tongue (contact with the lower incisors).
The control group has positioned the tongue in different position.
Results study 1 All the subjects, who present muscular imbalances and hypertones at the first examination, rebalanced the values of the various muscles tested (oral, dorsal and paravertebral muscles) as soon as the tongue was placed in contact with the palatine receptors. The positioning of the tongue in different places did not give similar results. Discussion From the analysis of the tests, the tongue shows to have a noticeable effect on the overall posture. This effect is mediated by the change and the rebalancing of the muscular tone through a better functional relationship between the various muscular chains.
Results study 2 The analysis of the values of 5hydroxydolacetic acid, catabolite of serotonin in the urine of 24 hours, allowed to highlight a greater production of serotonin with the exercises of positioning the tongue in contact with the spot. Discussion Studies are confirmed that serotonin deficiency is implicated in the appearance of juvenile idiopathic scoliosis.
Introduction
Many researchers have recognized a multiplicity of ethiological causes [2] giving importance, based on their cultural background, to the visual system, the vestibular system, occlusion, neuromuscular or developmental problems, endocrine disorders, genetic.
The role of serotonin and melatonin in scoliosis is controversial. [3,4,5,6,7,8,9]. In fact, specific receptors for these substances have been found along the entire spinal column. However, no one has analyzed other elements correlated with the alterations of these two substances.
We leave out the general and biochemical mechanisms related to melatonin. Let’s just remember that Melatonin and Serotonin are produced by the pineal gland. Serotonin is produced during the day, Melatonin at night, in the dark and in sleep.
The initial studies of the relationships between the pineal gland is mainly due to the research of Machida and others who created scoliosis in chickens through the ablation of the pineal gland. [10, 11].
Being a gnathologist and orthodontist and having been interested in the rehabilitation of orofacial muscles and swallowing in my treatments for thirty years, I soon realized changes in posture obtained “involuntarily” in patients who practiced myofunctional therapy as a support and prologue to specific oral treatments. (fig.1,2)
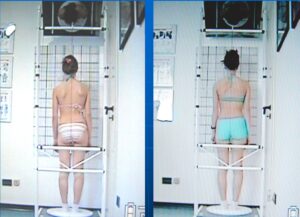
Fig 1 Patient before MFT Fig 2 After MFT
For many years I searched for an explanation for what I saw very often: patients improved in orofacial muscular balance, but also, almost always, in postural attitudes and scoliosis [12] during the swallow rehabilitation.
However I could find no explanation. Then, I happened to read a research conducted in various animal species by Halata and Baumann [13], who had discovered the presence, at the emergence of the naso-palatine nerve (II trigeminal branch), of the five exteroceptors most present in the human body.
At this point I must explain that the naso-palatine hole (fig.3,4) (defined Spot in Myofunctional therapy) is considered the point of support of the tongue on the palate during

Fig 3 Palatine hole Fig 4 Nose-palatine Nerve
physiological swallowing. In subjects presenting an incorrect swallow, stimulation of the aforementioned receptors is almost always decreased or lacking. Many are the causes of alterations in swallowing mechanics. [14] The numerically most important reason is feeding with artificial methods. In breastfeeding the newborn unconsciously learns to swallow with the pressure of the tongue against the palate, compressing the nipple to obtain the squeezing. In bottle feeding, the newborn is forced by the teat to a low tongue position and learns to use only the lingual muscles with a horizontal function, losing the ability to lift the tip of the tongue in contact with the palate. In this case the tongue will become inefficient for swallowing and will be replaced by the buccinator muscles. These are able to help swallowing, but cause problems both on the structure of the jaws and in even distant areas. Other causes are given by birth compressions of the hypoglossal nerve during natural childbirth and anatomical problems such as a very short frenulum and ankylotic tongue. If stimulation of the palatine receptors in the dysfunctional patient can only be impeded or diminished, in the patient with ankyloglossia it is completely prevented. I remember that the anatomical alterations of the tongue are genetic and often the patient with ankylotic tongue presents scoliosis [15], but no one has referred to this type of genetics.
About 70% of the cases of patients with scoliosis that belong to my office have alterations in swallowing accompanied by malocclusions and associated muscle imbalances. It is often possible, by measuring the masseters, to understand what is the alteration of tone in the spine and the type of curve that we can find.
For many years we have tried to explain the relationship between swallowing and postural alterations, but only the discovery of the naso-palatine receptors has given an impetus to our research. Being a teacher in many Masters in Posturology I was able to assign theses on topics that are not part of the dentist’s cultural background and expand my knowledge on mouth-brain relationships.
The first thing observed was clear. If the attitude and the curves of the spine improved, it was evident to me that the tone of paravertebral and of the trunk musculature was balancing. Lacking research on the subject, I managed to get my son, graduating in Medicine, assigned a thesis on changes in the tone of the paravertebral muscles and trunk by varying the position of the tongue. [16]
Study design 1
Materials and methodologies
In our research we used Electromyograph Myo-tronics Inc. to measure the stomatognathic and trunk muscles, Myometer, to evaluate the function of the tongue and masseter muscles, Black light lamp and Fluorescein in sepigel 1% to evaluate the lingual dynamics during the swallowing act.
40 subjects were tested, all in good health, aged between 18 and 25 years, both genders, with the only common factor of the presence of an incorrect swallowing and an altered tongue posture evaluated through the use of Fluorescein sepigel 1 %. The examination allowed to evaluate the correctness of the tongue movement during the swallowing act detecting the presence of Fluorescein (visible in the mouth through the Wood’s lamp). Once the fluorescein is applied on the lingual apex and on the upper edges of the zone corresponding to the premolars and the spontaneous swallowing of the patient is done, the areas where the Fluorescein appear are detected. In a physiological environment three small round areas are found on the tongue and on the palate, only on the palatine Spot and in the lateral region of the palate at the level of the premolars. In patients with dysfunction of the swallowing coloured streaks can be found on the tongue and colour deposited in places where the tongue touches the oral structures, that is, between the teeth, against the teeth or even on the inner side of the cheeks. Subjects with a short frenulum, spinal disorders or muscular diseases of any kind were excluded. Three evaluations were carried out: the first one with the tongue in habitual wrong position, the second with the tongue resting on the palate at the level of emergence of naso-palatine nerve, and the third positioning the tongue in a different way (against the lower incisors) assessing through the electromyography any potential changes.
In particular, the use of the surface electromyography for this purpose is recognized by the work of many experts of the spinal column and the scoliotic pathologies [19,20,21,22].
WORKING GROUP: N = 40 subjects aged 18-25 years not suffering from diseases of the spine, submitted to postural basic examination and electromyography at rest.
Rescreened with the same parameters after placement of the tongue at the level of the spot Palatine (emergence of the nasal-palatine nerve)
CONTROL GROUP: The same 40 patients constituted the control group, examined after the underlying condition, with different positioning of the tongue (contact with the lower incisors).
Results
Electromyography
Using a surface electromyography it has been evaluated the activity in rest conditions of certain head and trunk muscles and their modifications following the repositioning of the tongue on the palatine spot. A control test was then carried out assessing the muscular activity by placing the tongue against the lower incisors.
Four pairs of muscles were evaluated:
Masseter, Sternocleidomastoid, trapezius and paraspinal muscles at the level of the third lumbar vertebra.
The recordings were made with patients in a sitting position and without that they were been made aware of what was expected by the outcome of the examination.
Below the reference values for each muscle and the standard deviations that allow defining the degree of activity:
Reference Range Standard deviation
Masseter 1.87 microVolts 1.46
Sternocleidomastoid 1.98 microVolts 1.75
Trapeiius 2.78 microVolts 3.03
Paraspinal L3 1.41 microVolts 1.62
Legenda
LMM – Left masseter muscle
LSC – Left sternocleidomastoid muscle
RSC – Right sternocleidomastoid muscle
RMM – Right masseter muscle
LTP – Left trapezius muscle
LPS – Left paraspinal muscle
RPS – Right paraspinal muscle
MTP – Right trapezius muscle
All the subjects, who present muscular imbalances and hypertones at the first examination, rebalanced the values of the various muscles tested (oral, dorsal and paravertebral muscles) as soon as the tongue was placed in contact with the palatine receptors, denoting an effect of an exquisitely neurological nature involving of the cerebellum which, we recall, receives trigeminal information in the paramedian part and lingual information in the cerebellar worm.
Results
The result of the example (fig. 5,6) is similar to that obtained in the other 39 subjects with minimal variations between the individual muscles. The positioning of the tip of the tongue in contact with the palatine receptors showed a clear and immediate effect in almost all the tested patients.
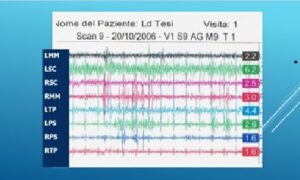
Fig 5 EMG with Tongue in habitual position
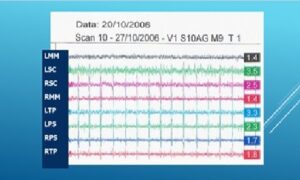
Fig. 6 EMG with Tongue to the Spot
Discussion
From the analysis of the tests, the tongue shows to have a noticeable effect on the overall posture. This effect is mediated by the change and the rebalancing of the muscular tone through a better functional relationship between the various muscular chains. From the tests it clearly appears an improvement in most of tested subjects. The cases that on the other hand showed a worsening or have improved much less than the others by placing the tongue on the Spot denoted a behavior similar to the presence of a short frenulum. The explanation is to be found in the stretching of the lingual muscles in an attempt to lighten the tongue against the palate in the presence of an anatomical impediment.
Conclusions
Research shows that the role of lingual posture and swallowing in people with muscle tension and pain problems cannot be overlooked. A careful analysis of these elements can help in interventions aimed at restoring the well-being of the patient with serious muscle tension otherwise inexplicable such as patients with fibromyalgia, in which knowledge of the damage created by the alteration in swallowing could help to understand the unexplainable symptoms from a physiatric or rheumatological point of view.
Study design 2
Another element was clear to me: if, as Machida et al. stated, adolescent idiopathic scoliosis was due to a deficiency of Melatonin and Serotonin, it could mean that, my patients that improved scoliotic curves during myofunctional treatment, perhaps had defects in the production of these neuromediators and that stimulation of the palatine receptors was able to normalize their production.
To validate this supposition, we carried out two studies by measuring the excretion of 5 hydroxy-indolacetic acid, which is a serotonin catabolite, in the urine during 24 hours.
The research group consisted of sixteen subjects between eight and sixteen years of both sexes (sixteen males and ten females). Ten subjects made up the control group. All presented with scoliosis and alterations in the swallowing mechanism. Subjects in the active group performed three-minute spot tongue placements, three times a day for thirty days.
Results
Working group
– in the male subjects 80,00% increased the serotonin concentration;
– in the female subjects 67,00% increased the serotonin concentration;
Control group
– in the male subjects 29% increased the concentration of serotonin;
– in the female subjects 47% increased the serotonin concentration;
– in the whole sample examined 40% increased their serotonin concentration;
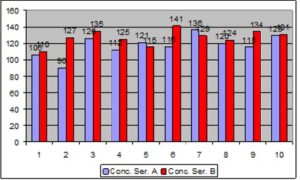
In 70% of scoliotic subjects, low serotonin values improved with palatine stimulation performed for three minutes three times a day. But already the stimulation of the palate for five minutes once a day was able to improve the excretion of this serotonin catabolite. [17, 18] (tab.1,2 ).
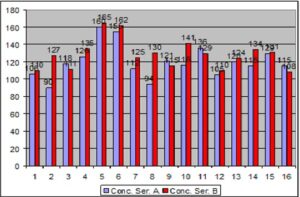
Tab. 1 Concentration in micrograms/24 hours of the initial and final serotonin in the male subjects of the study group. Blue histograms represent the first collection while red histograms indicate the second collection.
Tab. 2 Concentration in micrograms/24 hours of the initial and final serotonin in the female subjects of the study group. Blue histograms represent the first collection while red histograms indicate the second collection.
The average of increase in subjects with AIS went from 119.88 to 128.56, This data makes us think a lot about the possibility that this Myofunctional Therapy, implemented to restore the correct lingual function, can participate in the regulation of serotonin and muscle rebalancing in subjects with scoliosis.
Changes in the control group were not significant (tab. 3)
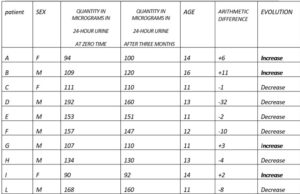
Tab.3 The non-significant changes in concentration in the control group
Conclusion
The analysis of the results that emerged from the studies leads to a single conclusion: probably the appearance and development of idiopathic scoliosis depend more on the muscular imbalance, caused by impaired swallowing, which also affects the spine, than on the lack of melatonin which reflects the poor stimulation of the palatine receptors. The fact that, however, even in the presence of a normal serotonin value, an improvement in its production is obtained by stimulating the palate, tells us that swallowing plays a role in both the onset of scoliosis and its healing.
Bibliography
1 Cheung Kenneth MC, Wang T,Qiu G X, Luk Keith D K: Recent advances in the aetiology of adolescent idiopathic scoliosis, Int Orthop 2008 Dec;32(6):729-
34.doi:1007/s00264-007-0393-y.Epub 2007 Jun 16
2 Girardo M, Bettini N, Dema e, Cervellati S,: The role of melatonin in the pathogenesis of adolescent idiopathic scoliosis (AIS) Eur Spine J. 2011 May;
20(Suppl 1): 68–74.
3 Bagnall KM, Raso VJ, Hill DL, Moreau M, Mahood JK, Jiang H, Russell G, Bering M, Buzzell GR. Melatonin levels in idiopathic scoliosis. 1997;21:1974– 1978. doi: 10.1097/00007632-199609010-00006.
4 Bagnall KM, Raso VJ, Hill DL, Moreau M, Mahood JK, Jiang H, Russell G, Bering M, Buzzell GR. Melatonin levels in idiopathic scoliosis. Diurnal and nocturnal serum melatonin levels in girls with adolescent idiopathic scoliosis. 1996;21:1974–1978. doi: 10.1097/00007632-199609010-00006.
5 Fagan AB, Kennaway DJ, Sutherland AD. Total 24-hour melatonin secretion in adolescent idiopathic scoliosis: a case–control study. 1998;23(1):41–46. doi: 10.1097/00007632-199801010-00009.
6 Hilibrand AS, Blakemore LC, Loder RT, Greenfield ML, Farley FA, Hensinger RN, Hariharan M. The role of melatonin in the pathogenesis of adolescent idiopathic scoliosis. 1996;21:1140–1146. doi: 10.1097/00007632-199605150-00004.
7 Machida M, Dubousset J, Imamura Y, Miyashita Y, Yamada T, Kimura J. Melatonin: a possible role in pathogenesis of adolescent idiopathic scoliosis. 1996;21:1147–1152. doi: 10.1097/00007632-199605150-00005
8 Machida M, Murai H, Miyashita Y, Dubousset J, Yamada T, Kimura J. Pathogenesis of idiopathic scoliosis. 1999;24:1985–1989. doi: 10.1097/00007632- 199910010-00004.
9 Machida M. Causes of idiopathic scoliosis. 1999;24:2576–2583. doi: 10.1097/00007632-199912150-00004
10 Machida M, Dubousset J, Imamura Y, Iwaya T, Yamada T, Kimura J. Role of melatonin deficiency in the development of scoliosis in pinealectomised chickens. J Bone Joint Surg (Br) 1995;77-B:134–138.
11 Machida M, Dubousset J, Imamura Y, Iwaya T, Yamada T, Kimura J. An experimental study in chickens for the pathogenesis of idiopathic scoliosis. 1993;18:1609–1615. doi: 10.1097/00007632-199309000-00007.
12 Ferrante A, Reed-Knight E, Bello A, Comentale P. Variazioni posturali conseguenti a cambiamento della posizione linguale ed a trattamento mio
funzionale; Ortognatodonzia italiana, vol. 11, 3 -2002
13 Halata Z., Baumann K.I.: “Sensory nerve endings in the hard palate and papilla incisiva of the rhesus monkey”; Anatomy and Embriology, vol.199, iss.5, pp
427-437,1999
14 Ferrante A, Terapia miofunzionale, dalla deglutizione atipica ai problemi posturali”, Futura Publ. Society, 1997
15 Ferrante A. Frenulo linguale corto. Centro Terapia miofunzionale.10/2017
16 Ferrante Alberto. Modificazioni posturali secondarie alla variazione di funzione di alcuni muscoli del capo e del collo. Seconda Università di Napoli. Anno
acc. 2005/2006
17 Locati F. Fedeli R. Correlazione tra deglutizione scorretta, secrezione di serotonina e scoliosi in età evolutiva. Università La Sapienza, Roma, anno acc.
2008/2009.
18 Tamburro S., Severino A., Nastro S.,Valutazione dei valori urinari di serotonina in ragazzi scoliotici, prima e dopo tre mesi di rieducazione della
deglutizione. Università Sapienza, Roma, anno acc. 2009/2010.
19 Avikainen VJ, Rezasoltani A, Kauhanen HA,:”Asymmetry of paraspinal EMG-time characteristics in idiopathic scoliosis”. J Spinal Disord. 1999
Feb;12(1):61-7.
20 Cheung J, Halbertsma JP, Veldhuizen AG, Sluiter WJ, Mauritz NM, Cool JC, Van Horn JR,: “A preliminary study on electromyographic analysis
paraspinal musculature in idiopathic scoliosis”. Eur Spine J. 2005 Mar;14(2):130-7. Epub 2004 Sep 11.
21 Gaudreault N, Arsenault AB, Lariviere C, De Serres SJ, Rivard CH: “Assessment of the paraspinal muscles of subjects presenting an idiopathic scoliosis: an
EMG pilot study”.BMC Musculoskelet. Disord. 2005 Mar 10;6:14.
22 Grassme R,Arnold D, Anders Ch, van Dijk JP, Stegeman DF, Linss W, Bradl I, Shumann NP, Sholle HCh: “Improved evaluation of back muscle SEMG
characteristics by modelling”. Pathophysiology. 2005 Dec;12(4):307-12. Epub 2005 Oct 25.
Dott. Antonio Ferrante
I° traversa Luigi Angrisani, 23
84014 Nocera Inferiore – Sa, Italia
e-mail dott.antonioferrante@gmail.com